

Abstract
Introduction: Multiple myeloma (MM) is a plasma cell neoplasm, characterized by plasma cell infiltration inside the bone marrow, secretion of monoclonal immunoglobulin (paraprotein), and end organ damage including lytic lesions in the bones. About 80-90% of myeloma patients suffer from osteolytic lesions during the course of the disease. 18F-FDG PET/CT is an imaging technique capable to detect active disease in patients in multiple myeloma (MM) and can be helpful in staging and prognosis. However, its routine use is still hampered by several factors, including high cost, reimbursement issues, lack of cost-effectiveness studies and limited availability. 99mTc-sestamibi (MIBI) has also been proposed as a potential tracer in MM evaluation and is more accessible with lower costs. The aim of this study was to compare these two imaging modalities at staging disease and their relation with clinical data.
Materials and Methods: Sixty-four patients with newly diagnostic MM (30 male; 34 female) were submitted to 18F-FDG PET/CT and 99mTc-Sestamibi SPECT/CT before treatment. Whole body PET/CT images were acquired 60 minutes after FDG administration and anterior and posterior whole-body scans (WBS) plus SPECT/CT of chest and abdomen were obtained 10 minutes after MIBI injection. Number of focal lesions, bone marrow involvement, contiguous soft tissue impairment and extra osseous lesions were recorded. Number of focal lesions was classified in 3 groups: 0 (no lesions); 1 (1-3 lesions); 2 (4-10); 3 (more than 10). A visual degree of uptake was defined for bone marrow involvement: comparison to liver on PET/CT and to myocardium on MIBI. Standardized uptake value (SUVmax) of the hottest lesion of each patient was registered. Potentials factors contributing to progression-free survival (PFS) were assessed with Cox regression model combining baseline clinical data (including renal function, anemia, hypercalcemia, LDH, bone marrow plasma cell percentage and ISS (I, II or III)) along with PET/CT and MIBI scan status.
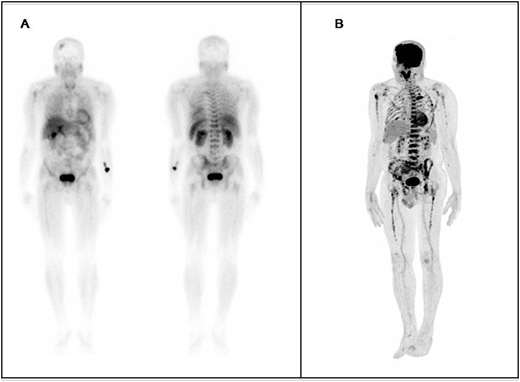
Results: PET/CT was positive in 61 patients (95%) and MIBI in 59 subjects (92%; P = 0.15). WBS was positive in 56 patients while WBS plus SPECT/CT was positive in 59 (p= 0.08). PET/CT detected extra osseous lesions in 4 patients and sestamibi in 1 subject. Contiguous soft tissue involvement was found in 29 and 24 patients on PET/CT and MIBI, respectively (p=0.05). PET/CT detected much more focal lesions than MIBI: 13, 11, 16 and 24 patients were in group 0, 1, 2 and 3 on PET/CT and 30, 18, 6 and 10 were on the same groups respectively on MIBI (p: 0.0001). In the figure below, a comparison between 99mTc-Sestamibi WBS (A) and 18F-FDG PET/CT (B) at staging in a 67 years-old male.
SUVmax were statistically different in subjects who presented elevated LDH (p= 0.02). Seventy-five percent and 100% of patients with elevated LDH had contiguous soft tissue involvement on MIBI and PET/CT respectively. More focal lesions on PET/CT were found in patients with hypercalcemia (p=0.02), however this correlation was not observed on MIBI (p=0.45). Renal insufficiency was a negative prognostic factor for PFS (HR: 2.25). The same was observed with advanced ISS staging (HR: 4.29). However, only advanced ISS staging (III) and extramedullary disease detected by MIBI were independent predictors of worse PFS.
Conclusion: There was no difference in the detection of active disease when comparing FDG PET/CT and MIBI SPECT/CT in MM staging, although the first one detected more number of lesions. Including SPECT/CT to planar images on MIBI did also not improve the number of positive scans. Elevated LDH and hypercalcemia were the only clinical parameters related to higher number of bone lesions while ISS staging (III) and extramedullary disease detected by MIBI were independent predictors of worse PFS. Our study demonstrated that sestamibi WBI detects less volume of disease compared to PET/CT, however it may substitute PET/CT in centers where it is not available or there is no reimbursement for MM staging.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal